
As surgical procedures on babies to release the upper lip frenulum are being carried out in rapidly growing numbers, it is important that what’s normal and what isn’t be better understood.
Often the interventions exacerbate the problems. Every day in social media support groups, messages appear from mothers expressing their regret for having opted for surgery to release ties in their babies’ mouths because things are now worse, not better. As well as a baby who will not latch at the breast, they now have a baby who will not feed from breast or bottle, is traumatised, and in pain, with wounds that may have bled profusely. Today, I read another similar account: following a tongue and lip-tie release: the baby now has oral aversion and is being fed by syringe. The mother feels guilty and exhausted, as well as being $3000 out of pocket after paying for surgery, breastfeeding support, and bodywork. A highly recommended and popularly respected ‘provider’ had lasered the ties.
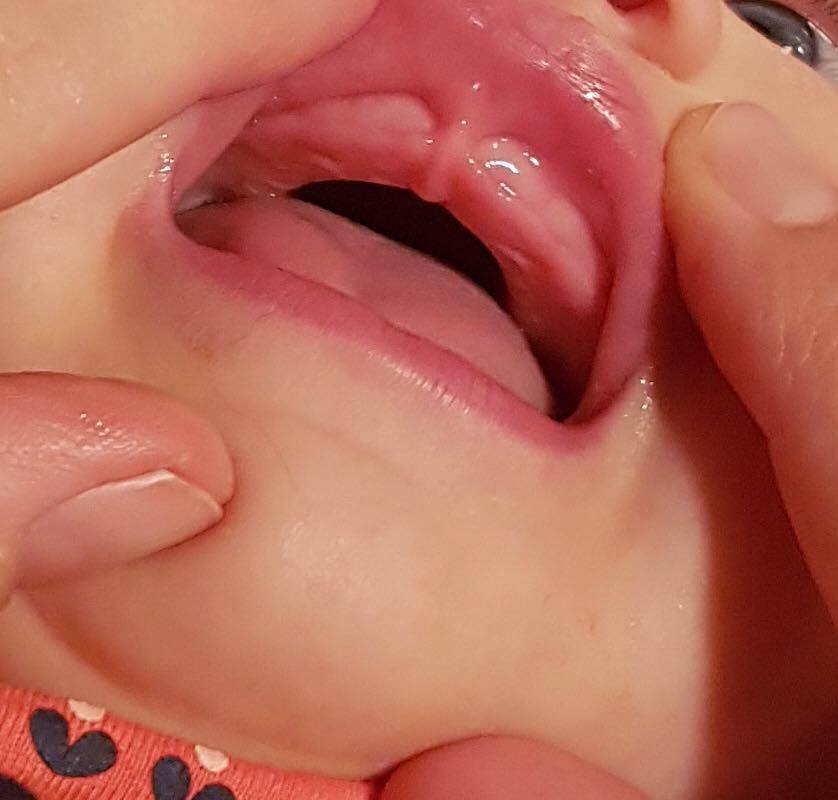 The superior labial (upper lip) frenulum is the soft tissue that attaches the upper lip to the gum. There is growing controversy on the identification, classification, and subsequent significance of this connective tissue, and when its presence constitutes a ‘lip-tie’. There are in fact a range of normal attachment sites of the superior labial frenulum.
The superior labial (upper lip) frenulum is the soft tissue that attaches the upper lip to the gum. There is growing controversy on the identification, classification, and subsequent significance of this connective tissue, and when its presence constitutes a ‘lip-tie’. There are in fact a range of normal attachment sites of the superior labial frenulum.
Previous research has shown that the attachment of the upper lip frenulum becomes noticeably less prominent with age. Also surgical removal of the upper lip frenulum in infancy may risk worsening any gap between the front teeth later in childhood, due to scarring.
 Despite the assumptions frequently related in social media and by a growing number of health professionals, it is not known whether the upper lip frenulum has any functional consequences relating either to its appearance or the degree of its attachment. Currently, the popular belief is that cutting or removing a prominent upper lip frenulum will help babies who are struggling to latch and feed at the breast. Such surgical intervention is being recommended, even where there are no problems with breastfeeding, as a preventative measure to protect against purely speculative future ramifications.
Despite the assumptions frequently related in social media and by a growing number of health professionals, it is not known whether the upper lip frenulum has any functional consequences relating either to its appearance or the degree of its attachment. Currently, the popular belief is that cutting or removing a prominent upper lip frenulum will help babies who are struggling to latch and feed at the breast. Such surgical intervention is being recommended, even where there are no problems with breastfeeding, as a preventative measure to protect against purely speculative future ramifications.
The upper lip frenulum has an extensive blood supply and many pain receptors. Cutting or lasering it inflicts pain. And doing so sometimes results in trauma and oral aversion. Infants have been admitted to hospital with haemorrhaging or other complications as a consequence of the procedure.
While there is no evidence that the intervention improves a baby’s ability to breastfeed, there has been an explosion in the number of surgeries being performed to cut or laser the upper lip frenulum (often together with the tongue’s frenulum). Recently, researchers at Stanford University conducted a prospective cross-sectional study aiming to shed light on what is the typical appearance in the newborn of the upper lip frenulum (Santa Maria, Aby, Trong, Thakur, Rea, & Messner, 2017).
An attempt to classify the frenulum has previously been made by Kotlow (2013) based on its appearance and location of insertion on the gum. The Kotlow classification system uses four grades to rate the frenulum (the higher the grade, the higher the ‘severity’ of ‘lip-tie,’ and the greater the association with breastfeeding problems. Kotlow described ‘lip-tie’ as a problem that interferes with an infant’s ability to flange the upper lip around the nipple and achieve a successful latch. Not so, says Professor Douglas. This year in her work with the Human Lactation Research Group, at the University of Western Australia, using ultrasound to illuminate the biomechanics of infant suck during breastfeeding, she confirmed that the upper lip does not need to flange for pain-free milk transfer. Kotlow’s classification scale has been (and is being) used as a clinical factor in decisions whether to release the frenulum, yet neither the relationship between grade of lip-tie and breastfeeding difficulty, nor clinical outcomes after lip-tie release, have been clearly demonstrated in any studies.
In the Stanford study (2017), using the attempted Kotlow classification system, relevant medical professionals rated the appearance of the upper lip frenula in 100 newborns using high-resolution close-up images that could be magnified and viewed in a controlled manner not possible when examining newborns directly. The study’s authors graded the images twice using the Kotlow system. They were blinded to the ratings of the other raters as well as their previous rating.
The results showed that all newborns have a superior labial frenulum. Raters had poor intra- and interrater reliability. The results identified very poor distinction between grades with a high degree of overlap. Only 8 of 100 photographs had the same rating all 12 times they were evaluated. Based on their analysis, they developed a new grading system to recalculate the results. Despite improved consistency with one grade fewer, the new system was still poor. Using either system, it is difficult to extrapolate to clinical significance frenulum function, or to justify procedures to remove the upper lip frenulum, when there is no consensus on category.
Since experts in the field cannot distinguish different types of upper lip frenulum, given the lack of knowledge surrounding its function, and the fact that all babies have one, releasing it based on appearance cannot be endorsed at this time.
Douglas dismisses posterior, buccal and upper lip-ties as a misconception. The diagnosis of ties creates pressure to intervene. New diagnoses should only be introduced with great caution because they are known to risk a cascade of overtreatment (Morgan, Brownless, Leppin, Kressin, Dhruva, Levin, et al., 2015; Saini, Brownlee, Elshaug, & Glasziou, 2017).
 Families are warned about various developmental risks of not proceeding with surgery, for instance, that without an operation the child may suffer feeding, speech, breathing, dental, postural and other problems, which frightens parents into compliance, though there is no evidence to support these claims. Because of the powerful impact of expectation, the chances of reported positive outcomes following laser surgery are increased (Brody & Miller, 2011). If you pay a large sum of money, or have an emotional investment, then you are not likely to admit (even to yourself) that you have been suckered.
Families are warned about various developmental risks of not proceeding with surgery, for instance, that without an operation the child may suffer feeding, speech, breathing, dental, postural and other problems, which frightens parents into compliance, though there is no evidence to support these claims. Because of the powerful impact of expectation, the chances of reported positive outcomes following laser surgery are increased (Brody & Miller, 2011). If you pay a large sum of money, or have an emotional investment, then you are not likely to admit (even to yourself) that you have been suckered.
 Tongue and lip-tie procedures are a lucrative source of income for the health professionals who perform them and consequently marketing strategies are well-funded and impressively persuasive. Parents desperate for a solution to their breastfeeding challenges are readily convinced by the repetition of reassuring messages. Many will be unaware of the poor methodologies and confounders in the research cited to convince them that cutting or lasering is the answer. When such surgeries have been carried out and the baby has gone on to breastfeed successfully, the mother willingly accepts that the surgery was the answer and may enthusiastically promote such intervention to others.
Tongue and lip-tie procedures are a lucrative source of income for the health professionals who perform them and consequently marketing strategies are well-funded and impressively persuasive. Parents desperate for a solution to their breastfeeding challenges are readily convinced by the repetition of reassuring messages. Many will be unaware of the poor methodologies and confounders in the research cited to convince them that cutting or lasering is the answer. When such surgeries have been carried out and the baby has gone on to breastfeed successfully, the mother willingly accepts that the surgery was the answer and may enthusiastically promote such intervention to others.
We shall have to wait and see during the next decade what exactly the repercussions will be for these baby guinea pigs. One paediatric dentist has mentioned how lip-tie surgery changes a baby’s facial appearance and not in an attractive way. She says, it is likely that the revised upper lip will rise up above the adult teeth in a somewhat horse-like fashion.
In September 2017, the Australian Dental Association Queensland President Dr. Gary Smith wrote expressing his fears in the ADA news bulletin:
‘New parents are often searching for an explanation to breastfeeding issues and will be influenced by professionals offering what seems to be a solution. We are in a powerful position as health professionals and we must exercise healthy scepticism and evaluate the evidence for everything we do. Anecdotal evidence just won’t pass muster … I am troubled by practitioners using social media to promote tongue and lip tie surgery … I think such exploitation of children is unconscionable and must cease.’
He pointed out that the International Affiliation of Tongue-Tie Professionals cites references as authoritative when Australia’s National Health and Medical Research Council cites the same references as very low quality based on no evidence.
The Cochrane review (2017) is clear:
‘It is uncertain whether ankyloglossia is a congenital anomaly requiring treatment or a normal variant.’
The small number of trials along with methodological shortcomings limit the certainty of findings in favour of surgical intervention. In fact, none of the research has been able to demonstrate that any of the mother-reported improvements are attributable to surgical interventions. In the case of a classic anterior tongue-tie tethering the tongue at its tip, a small snip to free it may have an immediate effect to allow a baby to achieve a better latch. If it doesn’t, then cutting it was not appropriate.
Douglas (2017) said:
‘Anything that directs parental financial resource and time investment away from the practice of optimal fit and hold [position and attachment] delays the critical repair of the disrupted breastfeeding relationship and is disempowering for women. Craniosacral and oral myofunctional therapy and related techniques simply cannot compare with healthy effects on postural alignment and functional musculoskeletal health achieved by optimal positional stability and fit and hold, repeated over and over for many hours each day. [Practice makes perfect.]’
Providers of breastfeeding care should respect that vulnerable babies depend on them to keep them safe from harm and that, says the ADA President, includes ‘holding off on surgery if no evidence exists to put them through it. If we simply follow dogma, the procedure could be considered on a par with circumcision or the docking of a dog’s tail.’
Editorial note. 2nd December, 2018. Interesting (and cheering) to read what Alison Hazelbaker, well-known specialist in infant sucking problems, who wrote one of the earliest books on tongue-tie, and created the Assessment Tool for Lingual Frenulum Function, is now saying about the ‘industry’ she helped ‘spawn’ (Her choice of words, by the way).
‘Co-opting the term tongue-tie to refer to acquired conditions, as has been done in the last decade and a half, undermines the entire concept and definition of tongue-tie, leading professionals and parents astray.
‘These days, tongue-tie refers to any visible frenum making the normal phenotype pathological. Any cause of tongue motion deficits is dubbed tongue-tie leading many babies to unneeded surgery (like cattle to slaughter.)’
‘The truth is that there is no scientific evidence that proves that prominent labial frena, “buccal ties” or any other form of (fabricated) tongue tethering causes any of the dysfunctions claimed to occur by the participants in this burgeoning industry.’ (See What’s in a name.)
In correspondence in August 2020, I wrote to Alison, ‘I hope you are encouraging parents not to mutilate their babies by cutting or lasering ties.’ She responded, ‘Of course! I have been the stand for stopping these heinous practices. At a great expense to my reputation.’
Editorial note. 13th August, 2018. Naini, F. B., & Gill, D. S. (2018). Oral surgery: Labial frenectomy: Indications and practical implications. BDJ, 225(3), 199–200. doi:10.1038/sj.bdj.2018.656 (‘undertaking a frenectomy too early and removing the interdental fibres leads to scar tissue formation, generating an obstacle which may lead to difficulties in subsequent diastema closure.’… ‘frenectomy is almost always contraindicated prior to orthodontic treatment…. ‘it is worth repeating that the simple presence of a labial frenum, or a maxillary dental midline diastema, should not be a habitual reason for referral or an unconsidered indication for frenectomy.’)
Editorial note. 1st December, 2017. Following concerns that there is an epidemic of over diagnosis and over treatment of tongue and lip-ties in the US, Canada and Australia, the Australian Dental Association Queensland (ADAQ) Council has approved a submission to the Dental Board of Australia requesting guidance for dental practitioners on tongue and lip tie surgery. There are no data to indicate any underlying changes in recent years in the prevalence of tongue-tie, it says. It expresses worry over those practising ‘at the fringe of dentistry’ who ‘have linked in their minds the release of lip and tongue ties to all manner of long term health issues’ in, for instance, orthodontics, speech, posture, and sleep. They refer to bias and self-promotion by practitioners who have made a considerable income and built their professional reputations from surgically treating tongue-tie and promoting others to do likewise [They name one popular US practitioner as an example]. ‘Not surprisingly, there are many half-truths and fallacies pushed by those who promote tongue tie surgery for financial gain.’ ADAQ News (December 2017) 643, 5-6.
References (Updated May 2021)
Brody, H., & Miller, F.G. (2011). Lessons from recent research about the placebo effect—from art to science. JAMA, 306(23), 2612. doi:10.1001/jama.2011.1850
Douglas, P. Untangling the tongue-tie epidemic. (2017). Retrieved from http://medicalrepublic.com.au/untangling-tongue-tie-epidemic/10813
Kotlow, L.A. (2013). Diagnosing and understanding the maxillary lip-tie (superior labial, the maxillary labial frenum) as it relates to breastfeeding. Journal of Human Lactation. 29(4),458–464.
Morgan, D.J., Brownless, S.B., Leppin, A.L., Kressin, N., Dhruva, S.S., Levin, L., Landon, B.E., Zezza, M.A., Schmidt, H. Saini, V., Elshaug, A.G. (2015). Setting a research agenda for medical overuse. BMJ 351, h4534. doi: https://doi.org/10.1136/bmj.h4534
Naimer, S.A., Israel, A., Gabbay, A. (2021). Significance of the tethered maxillary frenulum: a questionnaire-based observational cohort study. Clin. Exp. Pediatr. Mar;64(3):130-135. doi: 10.3345/cep.2020.00486. (A tethered labial frenulum is not associated with an increase in breastfeeding disturbances or oral disorders. These data encourage clinicians to question the need to intervene in cases of tethered maxillary frenula.)
Nakhash, R., Wasserteil, N., Mimouni, F.B.,Kasirer, Y.M., Hammerman, C., Bin-Nun, A. (2019). Upper lip tie and breastfeeding: A systematic review. Breastfeeding Medicine, https://doi.org/10.1089/bfm.2018.0174 (Routine upper lip tie release cannot be recommended. The classification system proposed by Kotlow is unreliable both in terms of inter and intraobserver agreement and in terms of predicting the severity of the breastfeeding difficulties.)
Santa Maria, C., Aby, J., Trong, M. T., Thakur, Y., Rea, S., & Messner, A. (2017). The superior labial frenulum in newborns: What is normal? Global Pediatric Health, 4, 2333794X17718896. http://doi.org/10.1177/2333794X17718896
Saini, V., Brownlee, S., Elshaug, A.G., Glasziou, P., Iona Health. (2017) Addressing overuse and underuse around the world. The Lancet,10090 105–107. doi:http://dx.doi.org/10.1016/50140-6736(16)32753-9.
Shah, S., Allen, P., Walker, R., Rosen-Carole, C., McKenna Benoit, M.K. (2021). Upper lip tie: Anatomy, effect on breastfeeding, and correlation with ankyloglossia. 2 Laryngoscope. May;131(5):E1701-E1706. https://doi.org/10.1002/lary.29140 (There was no correlation between maxillary frenulum grade and comfort with breastfeeding, pain scores, or latch. There was also no relationship between tip to frenulum length (tongue tie) and visualized lip anatomy, suggesting that tongue tie and lip tie may not cluster together in infants.)
Smith, G., Australian Dental Association Queensland President (September 2017) ADA News Bulletin.
A list of my blog posts
Always Ask Questions: Don’t Let Your Tongue Be Tied
Censorship on Tongue-Tie. Whose Tongues Are Tied?
Did Tongue-Tie Release Fail to Improve Problems?
Does Tongue-Tie Disempower Mothers and Damage Babies?
How Credible Is The Current Oral Tie Trend?
Is The Current Breastfeeding Problem a Fault in Babies’ Mouths?
Is The Treatment of Tongue-Tie an ‘Unjustified Enthusiasm’?
Reading Between the Lines Post-Tie Surgery
Snipping Tongue-Ties. Whose Business?
Spinning a Web: Spiders and Tongue-Ties
Surgery on Babies: Does it Hurt?
The New Sucking Model and Tongue-Tie
Tongue-Tie and Infant Formula Milk Promotion
Tongue-Tie Epidemic Poses Risk to Community
Tongue-Tie Politics of Breastfeeding
When Releasing Tongue-Ties Does Not Fix Breastfeeding
Who Diagnoses Tongue-Ties that Interfere With Breastfeeding?
Why Upper Lip-tie Isn’t a Thing
There’s a Facebook group Evidence based tongue and lip tie information that may help mothers and health professionals make better sense of the research to inform their decisions.
Of interest so am reproducing here:
Australian Collaboration for Infant Oral Research (ACIOR)*
ACIOR Position Statement 1
4 October 2017:
Upper lip-tie, buccal ties, and the role of frenotomy in infants
Morphology
What are the maxillary labial and buccal frena?
The word frenum derives from the Latin frēnum, meaning ‘bridle’. Frēnulum is the diminutive of frēnum, meaning ‘little bridle’. The terms frenum and frenulum may be used interchangeably when discussing intra-oral connective tissue. In this statement, we use the term frenum.
A frenum is a small fold of tissue that secures or restricts the motion of a mobile organ, functioning anatomically as a protective connective tissue anchor, or tether, or tie. Frena are found in various parts of the body.
In the mouth, frena tether the lips to the gum, and the tongue to the floor of the mouth. These include the maxillary labial frenum and the laterally positioned buccal frena.
The midline maxillary frenum is made up of loose connective tissue, dense collagen, elastic fibres and epithelium. Sometimes it also contains muscle fibres, but these are usually few and located outside of the frenum proper.1, 2
The buccal frena are small connective tissue folds between the buccal mucosa and the gums, located lateral to the maxillary frenum, typically between the canines and premolars.
This Position Statement does address frena abnormalities associated with genetic orofacial syndromes, which require specialised treatment.
What is the functional relevance of the maxillary labial and buccal frena?
The wide range of maxillary labial and buccal frena morphologies do not tether or tie the lip in a way that impacts on function.3-5 The infant’s upper lip does not need to flange for effective breastfeeding. The upper lip participates in a neutral position in the seal created by the lower half of the face when the breastfeeding infant’s face buries symmetrically into the breast. The upper lip is not actively involved in effective milk transfer in breastfeeding, and is not visible when optimal intra-oral breast tissue volume and positional stability of the infant during breastfeeding are achieved.3-5
How should maxillary labial frena be classified?
Since the diverse range of maxillary labial morphologies do not impact upon function, there is no reason to classify variants as ‘upper lip ties’. The Kotlow scale and other systems for
classification of the maxillary labial frena (see Appendix), including the Stanford classification, are of anatomic interest, but lack clinical relevance.6, 7
How should buccal frena be classified?
Since buccal frena do not impact upon function, there is no reason to classify variants as ‘buccal ties’.
Why is this topic of concern?
Currently, health professionals diagnose variants of maxillary labial and buccal frena as abnormal in infants with breastfeeding problems or unsettled behaviour, and refer to dentists or other providers for ablation or incision with either laser or scissors frenotomy. Parents are advised to follow-up with wound stretching exercises multiple times a day for two or more weeks. Parents may also be advised to undertake a course of myofunctional or craniosacral therapy, which requires stretching and massage of the infant’s oral connective tissues and muscles a variable number of times a day.
There is no evidence to suggest that frenotomy of variants of maxillary labial and buccal frena helps with breastfeeding problems or protects against hygiene difficulties and anterior incisor decay in later childhood, despite claims.6, 8, 9
Although providers of oral surgery claim that pre-post surveys and chart reviews demonstrate the efficacy of the diagnosis and surgical treatment of upper lip-tie,10-15 these represent only Level IV evidence in the NH&MRC hierarchy and do not prove causal links.16 Providers of frenotomy have also argued that infants with an upper lip-tie or tongue-tie swallow more air when breastfeeding, causing stomach distention, crying behaviours, and reflux. However, studies that support this claim are methodologically weak, demonstrating interpretive bias.16, 17
What are the risks of maxillary labial and buccal frenotomy?
In the absence of relevant studies, we draw on expert clinical experience and anecdotal reports to list risks in order of clinical significance.
- Haemorrhage if scissors frenotomy (mitigated by use of laser)18
- Unnecessary pain and distress
- Wound infection19
- Oral aversion resulting in worsened feeding problems in infant with pre-existing breastfeeding or feeding problems
- Underlying feeding/breastfeeding problems remain unidentified and unmanaged
- Worsened diastema of upper incisors in later childhood due to scarring
What is appropriate, evidence-based management of maxillary labial and buccal frena?
We recommend no intervention, as maxillary labial and buccal frena are normal anatomic variants and do not ‘tie down the upper lip’ to impact on breastfeeding or feeding function. Unnecessary anxiety is created for parents when a normal anatomic variant is labelled as a ‘tie’.
The presence of what may appear to be a prominent midline maxillary frenum in infancy is not predictive of spacing between permanent maxillary central incisors. If a significant diastema emerges in later childhood, intervention may be appropriate at that time.
ACIOR Position Statement 1 Summary:
Upper lip-ties, buccal ties, and the role of frenotomy in infants
- In infants, maxillary labial and buccal frena:
- a) demonstrate a wide range of normal anatomic variation
- b) do not impact upon function, including in breastfeeding
- c) are not appropriately labelled as ‘upper lip ties’ or ‘buccal ties’.
- There is no role for frenotomy of maxillary labial or buccal frena in normal infants
- In the absence of benefit, frenotomy for maxillary labial and buccal frena poses unacceptable risk.
Appendix
Aetiology
Embryologically, the oral frena develop from central cells of the vestibular lamina. The maxillary labial frenum originates from the tectolabial bands, which appear at three months in utero and connect the tubercle of the upper lip with the palatine papilla. As the lateral halves of the alveolar ridge fuse, the bands are divided, forming the palatine papilla palatally and the labial frenum labially.1, 20, 21
The position of the maxillary labial frenum shifts apically as the alveolar process develops and moves coronally.1, 22 Commonly, the maxillary labial frenum inserts at the mucogingival junction but individual variations are marked.23-25 The relative shape and size of the maxillary labial frenum change with age and variations among individuals are also substantial.24-26 In line with the migration of the maxillary labial frenum with age, the width of any presenting diastema also commonly decreases from infancy to early childhood, but this may vary again when children reach the mixed-dentition stage.27
Classification of maxillary labial frenum
Sewerin (1971) classified the frenum according to morphological variations into “normal, normal with a nodule, normal with appendix, normal with nichum, bifid labial frenum, persistent tectolabial frenum, double frenum and wider frenum”.28
Mirko et al (1974) classified frena by position of insertion and attachment:23
- Mucosal – frenal fibres attached to mucogingival junction
- Gingival – frenal fibres inserted in attached gingiva
- Papillary – frenal fibres extended into interdental papilla
- Papilla Penetrating – frenal extended to palatine papilla.
Mirko et al reported that mucosally attached frenum were the most common in adults and papillary attached frenum were the least common.23
Classification of maxillary labial frenum alters with development
Boutsi and Tatakis in 2011 utilized Mirko’s classification in their study of different types of maxillary labial frenum in 226 children, aged 1-18 years, and concluded that “age differed significantly among children with different type of frenum attachment (p=0.0006)”. Older children were more likely to have mucosally attached frenum whereas the youngest children were more likely to have papillary penetrating frenum. They did not find any gender or ethnic differences.24 The findings from Lindsey et al., which examined 1285 English infants, children and adults, and those from Popovich et al. concur with the results of Boutsi and Tatakis, namely that apical migration of the maxillary labial frenum occurs with increasing age in children.29
Very occasionally, in the case of a frenum which is exceptionally large, or when the frenal attachment fails to migrate sufficiently, a persistent band of tissue is observed at or crossing the alveolar ridge crest and between the central incisors. It is possible that this may be associated with hygiene-related, anatomical and aesthetic concerns in later childhood and adulthood e.g. gingival margin retraction, dental plaque retention, diastema, lip or vestibule restrictions.1, 8, 24 In these rare cases, frenotomy may be of benefit, but this decision is made in later childhood or early adulthood, not in infancy.
*ACIOR members
Dr Pamela Douglas MBBS FRACGP IBCLC PhD ACIOR Co-ordinator, Medical Director, The Possums Clinic, Highgate Hill, Brisbane, Queensland, Senior Lecturer, Discipline of General Practice, The University of Queensland Adjunct Associate Professor, Maternity Newborn and Families Research Collaborative MHIQ, Griffith University
Associate Professor Angus Cameron BDS (Hons), MDSc, FDSRCS, FRACDS, FICD, FADI Staff Specialist, Paediatric Dentistry, Westmead Hospital Clinical Associate Professor, Paediatric Dentistry, University of Sydney
Dr Julie Cichero BA BSpThy Hons PhD Honorary Senior Fellow, School of Pharmacy, The University of Queensland; Adjunct Professor, School of Clinical Sciences, Queensland University of Technology; Co-Chair International Dysphagia Diet Standardisation Initiative
Associate Professor Donna Geddes DMU PGDipSc PhD Head of the Hartmann Human Lactation Research Group, School of Molecular Sciences, University of Western Australia
Associate Professor Peter Hill BA MBBS BHAdm FAFPHM Division Head, Health Systems and Policy, School of Public Health, The University of Queensland
Dr Vishal Kapoor MD FRACP MClinEpi Senior Staff Specialist in Paediatrics, Lady Cilento Children’s Hospital Senior Lecturer, School of Medicine, The University of Queensland
Dr Craig A McBride MBBS FRACS Senior Staff Specialist Paediatric Surgeon, Children’s Health Queensland Senior Lecturer, School of Medicine, The University of Queensland Adjunct Research Fellow, Griffith University
Winthrop Professor Marc Tennant BDSc PhD AFCHSE School of Human Sciences, The University of Western Australia
Dr Annetta Tsang BDSc(Hons) GCClinDent GCEd(HE) MScMed(Pain Mgt) DClinDent(Paed Dent) PhD Paediatric Dentist
Professor Laurie Walsh BDSc (Hons) PhD DDSc GCEd(HE) FRACDS FFOP (RCPA) FICD, FADI Specialist in Special Needs Dentistry
School of Dentistry, The University of Queensland
References
- Henry SW, Levin MP, Tsaknis PJ. Histologic features of the superior labial frenum. Journal of Periodontology. 1976;47(1):25-28.
- Ross RO, Brown FH, Houston GD. Histological survey of the frena of the oral cavity. Quintessence International. 1990;21:233-237.
- Douglas PS, Geddes DB. Practice-based interpretation of ultrasound studies leads the way to less pharmaceutical and surgical intervention for breastfeeding babies and more effective clinical support. 2017: under review.
- Douglas PS, Keogh R. Gestalt breastfeeding: helping mothers and infants optimise positional stability and intra-oral breast tissue volume for effective, pain-free milk transfer. Journal of Human Lactation. 2017;33(3):509–518.
- Thompson RE, Kruske S, Barclay L, Linden K, Gao Y, Kildea SV. Potential predictors of nipple trauma from an in-home breastfeeding programme: a cross-sectional study. Women and Birth. 2016;29:336-344.
- Kotlow L. Diagnosing and understanding the maxillary lip-tie (superior labial, the maxillary labial frenum) as it relates to breastfeeding. Journal of Human Lactation. 2013;29:458-464.
- Santa Maria C, Aby J, Trong MT, Thakur Y, Rea S, Messner A. The superior labial frenulum in newborns: what is normal? Global Pediatric Health. 2017;4(1-6).
- Kotlow LA. The influence of the maxillary frenum on the development and pattern of dental caries on anterior teeth in breastfeeding infants: prevention, diagnosis and treatment. Journal of Human Lactation. 2010;26(3):304-308.
- Douglas PS. Making sense of studies which claim benefits of frenotomy in the absence of classic tongue-tie Journal of Human Lactation. 2017;33(3):519–523.
- Benoiton L, Morgan M, Bauley K. Management of posterior ankyloglossia and upper lip ties in a tertiary otolaryngology outpatient clinic. International Journal of Otorhinolaryngology. 2016;88:13-16.
- Pransky SM, Lago D, Hong P. Breastfeeding difficulties and oral cavity anomalies: the influence of posterior ankyloglossia and upper-lip ties. International Journal of Otorhinolaryngology. 2015;79:1714-1717.
- O’Callahan C, Macary S, Clemente S. The effects of office-based frenotomy for anterior and posterior ankyloglossia on breastfeeding. International Journal of Pediatric Otorhinolaryngology. 2013;77:827-832.
- Siegel S. Aerophagia Induced Reflux in breastfeeding infants with ankyloglossia and shortened maxillary labial frenula (tongue and lip tie). International Journal of Clinical Pediatrics. 2016;5:6-8.
- Ghaheri BA, Cole M, Fausel S, Chuop M, Mace JC. Breastfeeding improvement following tongue-tie and lip-tie release: a prospective cohort study. Laryngoscope. 2017;127:1217–1223.
- Kotlow LA. Infant gastroesophageal reflux (GER): benign infant acid reflux or just plain aerophagia? International Journal of Child Health and Nutrition. 2016;5:10-16.
- Vassar M, Holzmann M. The retrospective chart review: important methodological considerations. Journal of Educational Evaluation for Health Professions. 2013:http//dx.doi.org/10.3352/jeehp.2013.3310.3312.
- Kaptchuk TJ. Effect of interpretive bias on research evidence. BMJ. 2003;326(1453- 1455).
- Tracy LF, Gomez G, Overton LJ, McClain WG. Hypovolemic shock after labial and lingual frenulectomy: a report of two cases. International Journal of Pediatric Otorhinolaryngology. 2017;100:223-224.
- Reid N, Rajput N. Acute feed refusal followed by Staphylococcus aureus wound infection after tongue-tie release. Journal of Paediatrics and Child Health. 2014;50:1030-1031.
- Huang WJ, Creath CJ. The midline diastema: a review of its etiology and treatment. Pediatric Dental Journal. 1995;17(3):171-179.
- Moore KL, editor. The Developing Human. 4th ed. Philadelphia: WB Saunders; 1988.
- Popvich F, Thompson GW, Main PA. The maxillary interincisal diastema and its relationship to the superior labial frenum and intermaxillary suture. Angle Orthodontist. 1977;47(4):265-271.
- Mirko P, Miroslav S, Lubor M. Significance of the labial frenum attachment in periodontal disease in man. Part 1. Classification and epidemiology of the labial frenum attachment. Journal of Periodontology. 1974;45(12):891-894.
- Boutsi EA, Tatakis DN. Maxillary Labial frenum attachment in children. International Journal of Paediatric Dentistry. 2011;21(4):284-288.
- American Academy of Pediatric Dentistry (AAPD). Guideline on management considerations for pediatric oral surgery and oral pathology. Revised 2015:Accessed online: http://www.aapd.org/media/Policies_Guidelines/G_OralSurgery2.pdf.
- Townsend JA, Brannon RB, Cheramie T, Hagan J. Prevalence and variations of the median maxillary labial frenum in children, adolescents and adults in a diverse population. General Dentistry. 2013;61(2):57-60.
- Diaz-Pizan ME, Lagravere MO, Villena R. Midline diastema and frenum morphology in the primary dentition. Journal of Dentistry for Children. 2006;73(1):11-14.
- Sewerin I. Prevalence and variations of the median maxillary labial frenum in children, adolescents and adults in a diverse population. Acta Odontologica Scandinavica. 1971;29(4):487-496.
- Lindsey D. The upper mid-line space and its relation to the labial frenum in children and in adults. A statistical evaluation. British Dentistry Journal. 1977;143(10):327-332.
